Your Thyroid Labs Are "Normal" — So Why Do You Feel Terrible?
- 4 days ago
- 9 min read
You're exhausted no matter how much you sleep. The weight won't move. Your brain feels like it's running through wet sand. You're cold when everyone else is fine. So you got your thyroid checked — and your doctor told you it's "normal."

It isn't your imagination, and you're not exaggerating. In most cases, the gland is making hormone exactly like it should. The failure is happening one step downstream — inside your cells, where inactive thyroid hormone is supposed to be switched on. Standard labs don't look there.
Here's what's actually going on, why two numbers on a blood test miss it, and what changes the picture.
The short version
Your thyroid mostly produces T4 — the inactive form of thyroid hormone. To do anything useful, T4 has to be converted into T3, the active form, by enzymes called deiodinases. That conversion is the bottleneck. When it stalls, you get every hypothyroid symptom in the book while your TSH and T4 sit in the "normal" column. The conversion stalls because the machinery that powers it — cellular energy and your antioxidant defenses — runs down with age, stress, and inflammation. Fix the upstream machinery and the downstream symptoms have a chance to resolve.

Why "normal" TSH and T4 don't tell you anything useful
Most thyroid panels check two things: TSH (a pituitary signal) and T4 (raw hormone in your blood). That's it. They confirm your gland is producing hormone and that it's circulating.
What they never check is whether your cells can convert that T4 into usable T3.
It's like confirming money is in your bank account but never checking that your debit card works. You can have plenty of T4 floating around and still be functionally hypothyroid at the cellular level — because the active hormone never gets made where it's needed.
According to the American Thyroid Association, an estimated 20 million Americans have some form of thyroid disease, and up to 60% don't know it. A two-marker panel is a big reason why.
The bottleneck: T4 → T3 conversion
The deiodinase enzymes that flip T4 into active T3 do their work mostly in your liver, kidneys, and peripheral tissues. They are selenium-dependent enzymes, and they don't run on goodwill. They need two things in steady supply:
NADPH — the cellular currency that powers the conversion reaction
Glutathione — your master antioxidant, which doubles as a required cofactor for the enzyme to function
Take either one away and throughput drops. Early deiodinase research from the 1980s showed how tight this dependency is: when researchers supplied NADPH to liver tissue, T3 production jumped several-fold — they described cellular energy as the rate-limiting step. Separate work showed that when glutathione was removed, conversion essentially stopped, and when it was added back, production climbed again. Cellular energy and antioxidant status aren't background details. They are the conversion.

The upstream driver: your cells are running on empty
Here's the part conventional testing never connects. The fuel for conversion is made in your mitochondria — the power plants in every cell — and it runs on a molecule called NAD⁺.
NAD⁺ peaks in your twenties and falls steadily after. By age 50, most people have lost a large share of what they had; by 60, considerably more. Less NAD⁺ means weaker mitochondria, less NADPH, and a deiodinase bottleneck — even when your gland is flawless and your T4 looks perfect.
Then modern life accelerates the drain. Chronic stress, broken sleep, ultra-processed food, gut dysfunction, infections, alcohol, heavy-metal and pesticide exposure, and several common medications all burn through glutathione and NAD⁺. Picture a 45- or 55-year-old professional under sustained load: natural production already down, reserves running on fumes. The gland is fine. The conversion is starved.
Reverse T3: when your biology protects you by shutting you down
This is where your own survival wiring turns against you — and it's the part that ties stress directly to your metabolism.
Start with a fixed amount of T4. Your body has to decide what to do with it: convert it into active T3, or convert it into reverse T3 (rT3) — a mirror-image molecule that fits your thyroid receptors but never switches them on. Think of it as a key that slides into the lock and won't turn.
That decision costs you twice. Every molecule of T4 redirected toward reverse T3 is one that never becomes active T3 — so you produce less usable hormone in the first place. Then the reverse T3 you did make crowds the active T3 you have left off its receptors. Less hormone made, and less of it able to act. Both ends of the equation working against you.

What decides the split? A signal. Your cells continuously report their conditions, and that status report sets the orders. When conditions are good, the body favors active T3 and runs metabolism at full output. When cells are depleted, inflamed, and energy-starved, a different enzyme — type 3 deiodinase — ramps up, shunting T4 toward reverse T3 and away from the active form. The message becomes: slow everything down to conserve resources for survival.
You've felt the everyday version of this. Think of the last time you had a bad cold or the flu — drained, foggy, no appetite, every signal telling you to lie down. That heavy feeling isn't only the virus; it's your body deliberately throttling its own metabolism to redirect energy toward fighting and repair. It's the same protective response that slows metabolism during serious illness or starvation. Smart, in the short term.
The problem is that in modern life the crisis signal never switches off. The stress is chronic and the depletion is constant — and your cells can't tell one kind of stress from another. Physical, psychosocial, environmental: it all registers as the same thing — threat. Each of these keeps the signal lit:
Physical: short sleep, blood-sugar swings from ultra-processed food, an inflamed gut, an old infection never fully cleared, hard training without real recovery.
Psychosocial: a high-demand career you won't slow down for, financial pressure, caregiving for children and aging parents at once, isolation, and stress that was never processed and still lives in the body.
Environmental: air pollution, pesticide residue and heavy metals in food and water, endocrine-disrupting plastics, mold in a water-damaged home or workplace, and late-night light exposure disrupting the sleep you were counting on.

Your body doesn't rank these inputs. It adds them up — and the total rarely drops low enough to call off the crisis. So your biology stays locked in conservation mode, throttling your thyroid at the cellular level while your bloodwork reads "fine."
This is also why your nervous system and immune system belong in any honest thyroid conversation, not as an afterthought. The signals that tell your cells "we're under threat" are psychoneuroimmune signals — stress physiology, inflammatory messengers like IL-6, and the cellular threat response itself.
IL-6 does three things at once:
it burns through NADPH,
it impairs the enzymes that make active T3,
it ramps up the enzyme that makes reverse T3.
Stress isn't a vague lifestyle factor here. It's a measurable biochemical driver of your thyroid output.
The vicious cycle, in one line
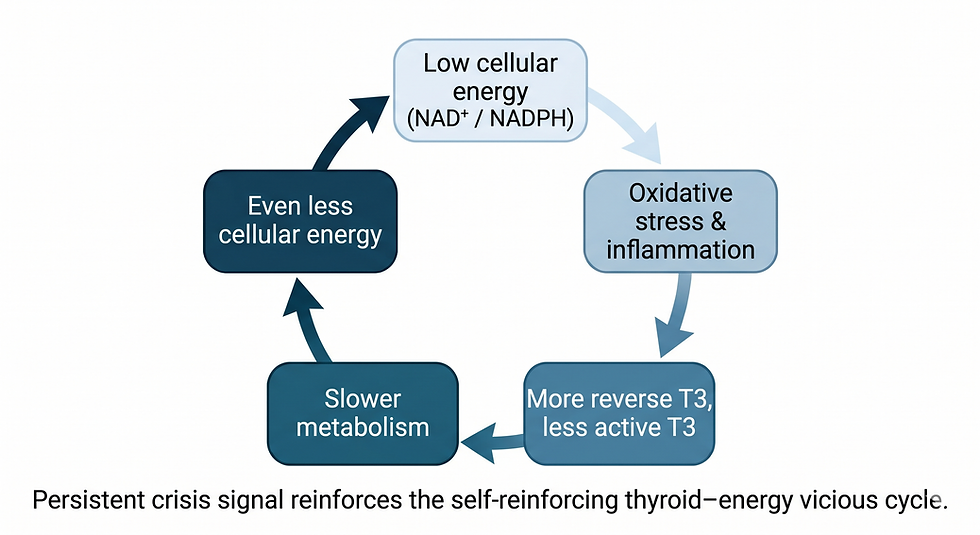
Low cellular energy → oxidative stress and inflammation → more reverse T3, less active T3 → slower metabolism → even less cellular energy.
Round and round. It explains why these symptoms tend to get worse over time even when your labs never budge.
What standard testing misses — and what to measure instead
If you only ever see TSH and T4, you are looking at two numbers and concluding the engine is fine because the fuel gauge reads full. A panel that can actually see the bottleneck includes:

Free T3 — the active hormone itself
Reverse T3 — the blocker
The Free T3 : Reverse T3 ratio — a direct read on conversion efficiency
Markers of oxidative stress and inflammation (including high-sensitivity CRP and IL-6) — the upstream drivers
Antioxidant and mitochondrial status — whether the machinery that powers conversion is intact
That's the difference between being told "everything is normal" and finally understanding why you feel the way you do.
Why you haven't gotten answers yet
If you've chased this for years without progress, it isn't because you didn't try. It's because the two places you'd turn for help fail in opposite directions.
Conventional medicine ignores the biochemistry. It measures TSH and T4, sees two numbers in range, and stops — no free T3, no reverse T3, no conversion, no cellular energy. The mechanism has been established in the literature for decades. It simply isn't part of a standard ten-minute appointment.
The wellness world oversimplifies it — and it rarely speaks with one voice, because each practitioner reads your symptoms through their own specialty and reaches for the tool they already use.
The nutritionist points to iodine.
The mindfulness coach points to breathwork and stress.
The biohacker points to NAD⁺.
The gut-health practitioner points to your microbiome.
The healthcoach points to adrenal stress
Each is holding a real piece of the picture. None is looking at the system that connects them.
That's the gap most people fall into: care that won't look deep enough on one side, single-lever fixes on the other. Thyroid function at the cellular level is a system — energy, antioxidants, inflammation, and conversion all moving together — and it has to be assessed and corrected as one.
What you can actually do about it
This isn't a single supplement or a single fix. The conversion bottleneck is held in place by four upstream problems, and you address them together.
1. Rebuild cellular energy (NAD⁺). The most powerful levers are free: regular exercise upregulates the enzymes that make NAD⁺ and builds healthier mitochondria, and time-restricted eating activates the same repair pathways. NAD⁺ precursors (NR, NMN) can help, but they're a supporting move, not a substitute for the work above.
2. Restore glutathione. N-acetylcysteine (NAC) supplies the rate-limiting amino acid; alpha-lipoic acid helps regenerate it; selenium is essential for both glutathione function and the deiodinase enzymes. Sulfur-rich foods — garlic, onions, cruciferous vegetables, quality protein — supply the raw material.
3. Quiet the inflammation. This is where the real leverage usually sits. Address gut dysfunction, protect deep sleep, and take stress physiology seriously — not as a wellness slogan, but as the direct input that drives IL-6 and reverse T3.
4. Support the mitochondria. CoQ10 for the electron transport chain, PQQ for building new mitochondria, magnesium and B-complex as core cofactors for energy production.
Give it time. Energy and mental clarity can shift within weeks; conversion markers usually take a few months to move, because you're rebuilding machinery, not flipping a switch.
Important: This is education, not a prescription. If you're on thyroid medication, do not change your dose without your physician. These strategies are meant to work alongside conventional care, not replace it.
How we work with this at The Johnson Center. Functional Health & Longevity
We don't run a two-marker panel and send you home. Through the Cellular Intelligence Protocol™ (CIP), we map the whole system — your full thyroid conversion picture, your inflammatory and oxidative load, your antioxidant and mitochondrial status, and the stress physiology driving all of it. Then we sequence the interventions in the order your biology needs them.
The entry point is the Cellular Baseline™ — a focused diagnostic that shows exactly where your conversion is breaking down and what's driving it. It's the difference between guessing and knowing.
[Book your Cellular Baseline™ →] · Virginia Beach · Blacksburg · Telemedicine across Virginia
Frequently asked questions
Can your thyroid labs be normal and you still have a thyroid problem? Yes. Standard panels measure TSH and T4, which confirm your gland is producing hormone. They don't measure whether your cells are converting that T4 into active T3. When conversion stalls, you can have textbook hypothyroid symptoms with "normal" labs.
What is T4-to-T3 conversion and why does it matter? T4 is the inactive form of thyroid hormone; T3 is the active form that drives metabolism, energy, and cognition. Enzymes called deiodinases convert T4 into T3, and that conversion requires cellular energy (NADPH), glutathione, and selenium. If conversion fails, circulating T4 never becomes usable hormone.
What is reverse T3 and what causes it to be high? Reverse T3 is an inactive form of thyroid hormone that occupies your receptors without activating them. It rises under chronic stress, inflammation, low cellular energy, illness, and prolonged caloric restriction — a survival mechanism that downshifts metabolism. Because every molecule of T4 diverted into reverse T3 is one that never becomes active T3, high reverse T3 means a double hit: more receptor blocking and less active hormone produced.
Why am I still exhausted if my TSH is normal? A normal TSH only tells you your pituitary sees enough T4 in circulation. It says nothing about whether your cells can convert and use that hormone. Fatigue with a normal TSH frequently points to a conversion problem driven by depleted cellular energy, low glutathione, and inflammation.
What thyroid tests should I ask for beyond TSH and T4? Free T3, reverse T3, and the Free T3 to reverse T3 ratio to assess conversion, plus markers of inflammation (hs-CRP, IL-6) and oxidative and mitochondrial status to identify what's driving the bottleneck.
Written by Dr. Barbara Johnson, MD — founder and medical director of The Johnson Center. Functional Health & Longevity. A former general/trauma surgeon with 20+ years in clinical medicine and 10+ years in Cellular & Longevity Medicine. Dr. Johnson built the Cellular Intelligence Protocol™ around a single principle: cellular energy controls health and longevity, and everything else is downstream.






































Comments